|
Welcome to part 2 of this investigation series! You can catch up on Part 1 right here. This investigation started with an immediate smoking gun! The pooling vessel had foaming issues and frozen broth chunks. The operators stuck a pool strainer into the tank to mix things up.  You read that right. They used a non-controlled pool strainer that’s not mentioned in any procedure. I still have no idea where it came from. They brought it through a CNC/ISO 9 transition zone, moved it through an ISO 9/ ISO 8 transition zone, opened the manhole entrance at the top of the tank, stuck it in the broth, then swirled it around for half an hour. When I interviewed the operators, they emphazied the exhorbitant amount of alcohol used to sanitize the tool in each transition zone. They wiped down each and every crevice, including inside the extension poles. But this was as obvious of a smoking gun as possible. We didn’t want to delay the start of the next engineering run (the last one scheduled). I wrote up the investigation report, also addressing a few extra potential contributors like maintenance performed on the mechanical transfer arm during the thawing process and an issue with the sample tubing. The report included all WFI, Environmental Monitoring (EM), and cleaning data proving the site and equipment were otherwise in control. All reviewers, including the Microbiology department head and the site Quality Assurance director, were happy with the report. It closed on time and the next run could move forward as planned. I watched that next engineering run with interest. Some self doubt crept in, and I had some perspective on the contamination that didn’t quite jive with the initial report. I snuck into the lab a day before the bioburden test plates were scheduled to be read. The plates looked the exact same as the previous run. Covered in Bacillus; >250 CFU/mL. Now things got scary. The site planned to run their first commecial batch in a month, but the previous two runs had overwhelming bioburden counts. A superstar team was put together.
This investigation had everything. It was treated with the intensity of a final product sterility failure, even though ~10 downstream bioburden samples were collected after further purification steps. We followed a DMAIC (Define, Measure, Analyze, Improve, Control) road map, with all the investigative tools you could ask for, like:
We even had another smoking gun that somehow didn’t come up during the first investigation! The first three engineering runs used a single pair of thaw vessels, the same pair each time. The 4th and 5th runs used both thaw vessel pairs (as seen in the overhead diagram). 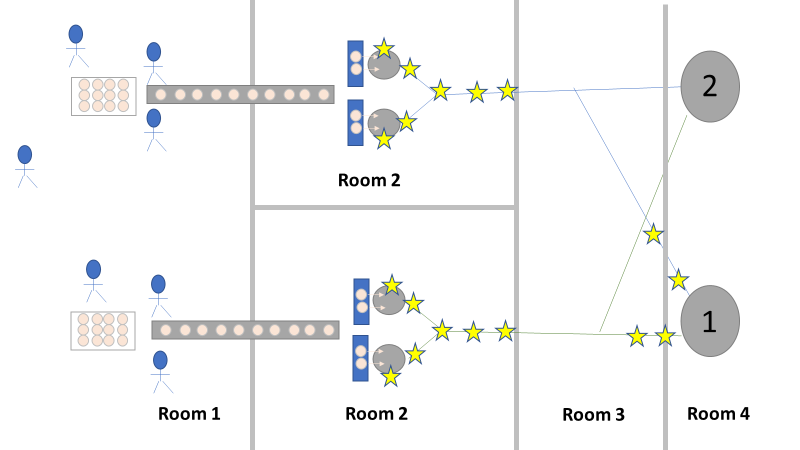 The organism had to be coming from this second thaw vessel chain, right? We thought so too, so we put together a major swabbing effort to see if we could find our bacillus organism. We swabbed both pairs of thaw vessels and the piping leading from them to to pooling vessel. We hoped the pair used for the first 3 runs would function as a control. The stars on the overhead diagram represent the approximate areas we swabbed. Keep in mind, all runs were performed using the pooling vessel marked “1”. The pooling vessel marked “2” (and the piping leading to it) was never used for these engineering runs. The Equipment CIP was performed soon after the 5th run was complete. Swabbing began a few days after the bioburden results were generated, so about a week passed between cleaning and swabbing. Guess what? We saw our Bacillus organism in almost every location we sampled. Both sets of thaw vessels. The counts were highest downstream near the pooling vessel, dwindling to a single colony (if any) on the thaw vessel rims. I gave a couple spoilers about non-root-causes in Part 1 of this series. My spoiler in Part 2: these results were accurate representations of what was swabbed. There were no sampling or testing errors that threw us off. As all raw material moved in a single direction through the equipment, the group came to the following conclusions:
Fortunately, both of those conclusions were dead wrong. Unfortunately, it took two rejected lots to figure that out. In the next part of this story, I’ll explain why the formulaic investigation techniques (i.e. the alphabet soup of techniques listed above) forced the investigation team to continue acting on those conclusions. I’ll also go into how the team should have been looking at this problem. This alternative mindset ended up saving a 3rd lot at the last minute. Check out Part 3, Part 4, and Part 5 here!
0 Comments
Leave a Reply. |
